Chairside 20
When an Unknown Abutment Is No Longer Acceptable
The patient presented with a referral letter. The referring dentist's note stated that the patient had an implant contraindication for the lower jaw due to bisphosphonate use; this contraindication was documented in the physician's letter as well. The patient also had a history of chest radiotherapy. From the very start, the implant was removed from the lower-jaw treatment path, and treatment shifted toward a removable partial denture.
The next question was whether the partial denture should be interim or definitive. Interim was set aside, because the logic of an interim prosthesis only holds when there is a defined time horizon — that is, when the physician has stated the contraindication holds until a specific date, after which it is reassessed. No such date had been set for this patient. An open-ended contraindication is, in practice, equivalent to a long-term one; so the decision moved toward a definitive partial denture.
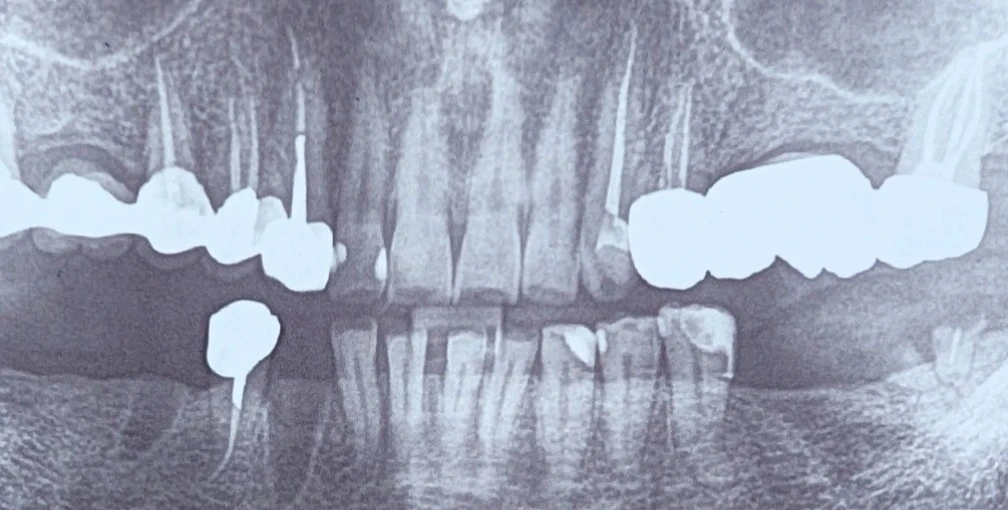
The first step was exactly what it should be: periapical radiographs of the abutment teeth. A panoramic is not sufficient for judging a single abutment; it does not provide apical, margin, and endodontic-quality information at the resolution needed.
Next we came to the crown on the lower-right tooth #4. The decision was to replace the crown, even if it looked radiographically ideal. The initial reasoning was mechanical: the crown has to align with the partial denture's path of insertion and removal, have a proper guide plane and rest seat, and the ferrule and the crown's own quality matter too. But none of these alone makes replacement mandatory — most of them can be corrected intraorally.
The real reason lay elsewhere. As a rule, no treatment is built over an unknown — and in this patient that rule only became stricter, because the patient's condition is more severe. In a patient on this medication, an abutment that later fails means extraction, and extraction is precisely the principal trigger of medication-related osteonecrosis of the jaw (MRONJ). So under an abutment that is going to bear load, no unknown is acceptable. A crown that is not known — whose post-and-core, ferrule, margin, and underlying decay status are unclear — cannot serve as an abutment expected to carry partial-denture forces for years. That is why the crown is opened and inspected: not because the partial denture's mechanics force it, but because in this patient the cost of failure is unacceptable.
The sequence toward this decision was as follows:
- Removing the implant from the lower-jaw treatment path, due to bisphosphonate use and a history of chest radiotherapy.
- Choosing a definitive partial denture over an interim one, since there was no contraindication with a defined time horizon.
- Obtaining periapical radiographs of the abutments for precise evaluation, rather than a panoramic.
- Deciding to open the crown on the lower-right tooth #4, not because of the partial denture's mechanical requirements, but to eliminate the unknown under a load-bearing abutment.
️No treatment should be built over an unknown — and the heavier the consequence of failure, the stricter this rule becomes, never looser.
️Bisphosphonate use did not create this rule; it only removed the margin of safety that usually allows an unknown to be overlooked.
The content of this page is intended for the educational use of dentists and dental students.